Peritoneal Vaginoplasty, also called the Peritoneal Pull‑Through Vaginoplasty (PPV), uses the thin, smooth peritoneal lining of the abdominal cavity to create the neovaginal canal. This laparoscopic, minimally invasive approach forms a moist, naturally contoured vaginal canal that resembles cis-female anatomy.

What Is PPV Vaginoplasty? Peritoneal Pull-Through Surgery at WIH by Dr. Chettasak
What is Peritoneum and Does Peritoneal Tissue Provide Self-Lubrication?
At WIH International Hospital, we offer Peritoneal Pull-through Vaginoplasty (PPV) as part of our advanced techniques for gender-affirming surgery and the treatment of vaginal agenesis. This approach utilizes a unique tissue from inside the abdominal cavity called the peritoneum, which is valued for its natural smoothness and hydration.
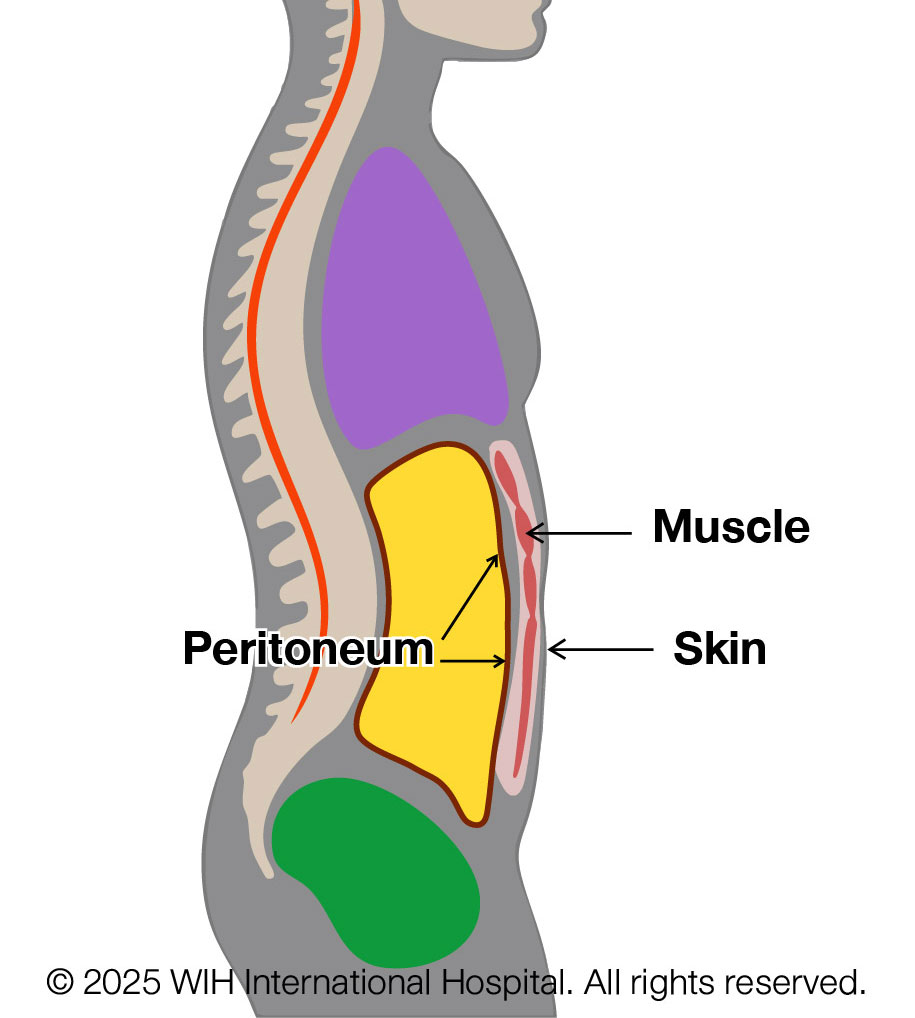
What is the Peritoneum?
The peritoneum is a thin, transparent membrane that lines the inner surface of the abdominal wall and wraps around organs such as the intestines, liver, and stomach. It acts like a protective inner lining — similar to wallpaper inside a room — allowing organs to move against one another smoothly and safely. One of the peritoneum’s natural functions is to produce a small amount of serous fluid that reduces friction during movement.
Because of its smooth, hydrated surface, the peritoneum has become a useful option in neovaginal construction, particularly for patients seeking a minimally invasive, bowel-free solution.
Does Peritoneal Tissue Provide Self-Lubrication?
Yes — the peritoneum naturally secretes serous fluid, a thin and clear substance that keeps its surface moist. When used in vaginoplasty, it contributes to the moisture inside the neovaginal canal. However, this fluid is not as thick or mucus-like as natural vaginal discharge or the secretions produced by colon tissue.
While peritoneal tissue does offer internal hydration, it does not provide strong resistance to friction. Therefore, patients who undergo PPV should continue using lubricating gel during dilation and sexual activity to maintain long-term comfort and prevent tissue trauma.
How Is the Peritoneum Used in Dr. Chettasak’s Hybrid NPI Technique?
At WIH, Dr. Chettasak Tulayaphanich has developed a hybrid technique that combines his signature NPI vaginoplasty with peritoneal pull-through. Instead of lining the entire canal with peritoneum, he uses skin graft for the distal portion near the vaginal opening — where friction is highest — and places the peritoneal flap in the deeper section of the canal.
This intentional hybrid design improves both durability and long-term aesthetic outcome, while taking advantage of the peritoneum’s moist characteristics in the deeper area. The peritoneal flap is harvested laparoscopically by our MIS team and integrated seamlessly into the neovaginal canal.
Although only the peritoneal segment produces natural moisture, our follow-up evaluations using per vaginal endoscopy have shown that the entire vaginal canal — including the skin-lined portion — can maintain a moist environment, providing adequate comfort for patients postoperatively.
Comparing Vaginal Construction Techniques: Skin Graft, PPV, and Colon Vaginoplasty
Each vaginoplasty technique has distinct characteristics in terms of self-lubrication and depth, and the choice depends on individual anatomy, goals, and medical considerations.
Vaginoplasty Technique Comparison
| Technique | Self-Lubrication | Typical Depth Achieved | Notes |
|---|---|---|---|
| Skin Graft Vaginoplasty | ❌ None – requires lifelong use of lubricating gel | 14–15 cm (5.5–6 inches) | Simple and effective, but dry |
| PPV (Peritoneal) | ✅ Yes – thin serous fluid (moist, but not mucous) | 15–17 cm (6–7 inches) | Laparoscopic, bowel-free option |
| Colon Vaginoplasty | ✅✅ Yes – thick mucous secretion (similar to natural vagina) | 18–20+ cm (7–8+ inches) | Best natural lubrication; involves bowel surgery |
Dr. Chettasak always provides individualized consultation to help each patient choose the method that best suits their expectations, anatomy, and long-term maintenance.
Benefits of PPV
• Moist, glistening lining with a smooth, natural texture
• Elastic and durable, promoting long‑term neovaginal integrity
• Minimal scarring due to laparoscopic access
• Optimal depth: ~6–7 inches (15–17 cm), sufficient for functional needs
When PPV Is Recommended
Ideal for patients who:
• Want a naturally moist canal without external grafts
• Lack sufficient genital tissue for skin‑graft methods
• Prefer a durable, low‑maintenance option without risk of deep graft shrinkage
• Seek laparoscopic surgery for quicker recovery and minimal scars
Why Is Laparoscopic Technique Required for PPV at WIH?
At WIH International Hospital, Peritoneal Pull-through Vaginoplasty (PPV) is performed using laparoscopic surgery — a minimally invasive approach that offers significant benefits for safety, healing, and long-term results.
Here are the top 3 reasons why the laparoscopic technique is essential — and why it’s part of our standard at WIH:
1. Safe and Gentle Harvesting of Peritoneum
The peritoneum is a thin, delicate membrane that lines the abdominal cavity. Using laparoscopy, our expert MIS surgical team can precisely harvest a wide, mobile sheet of peritoneum under direct vision — reducing the risk of damage to surrounding organs and significantly lowering the chance of internal adhesions (scar tissue formation).
2. Faster Recovery with Minimal Scarring
With only a few small incisions — usually hidden around the belly button and lower abdomen — laparoscopic surgery results in less pain, faster healing, and minimal visible scars. Patients recover more comfortably and enjoy better cosmetic outcomes without the trauma of traditional open surgery.
3. Proper Positioning for Long-Term Success
Laparoscopic access allows us to fully mobilize and orient the peritoneal flap deep inside the pelvis. This ensures that the tissue lines the neovaginal canal in a tension-free, natural configuration — helping to maintain proper depth, reduce complications, and support long-term function and satisfaction.
At WIH, our laparoscopic technique is carried out by a dedicated team of minimally invasive surgeons who work seamlessly with Dr. Chettasak to deliver exceptional results — combining precision, safety, and innovation in every procedure.
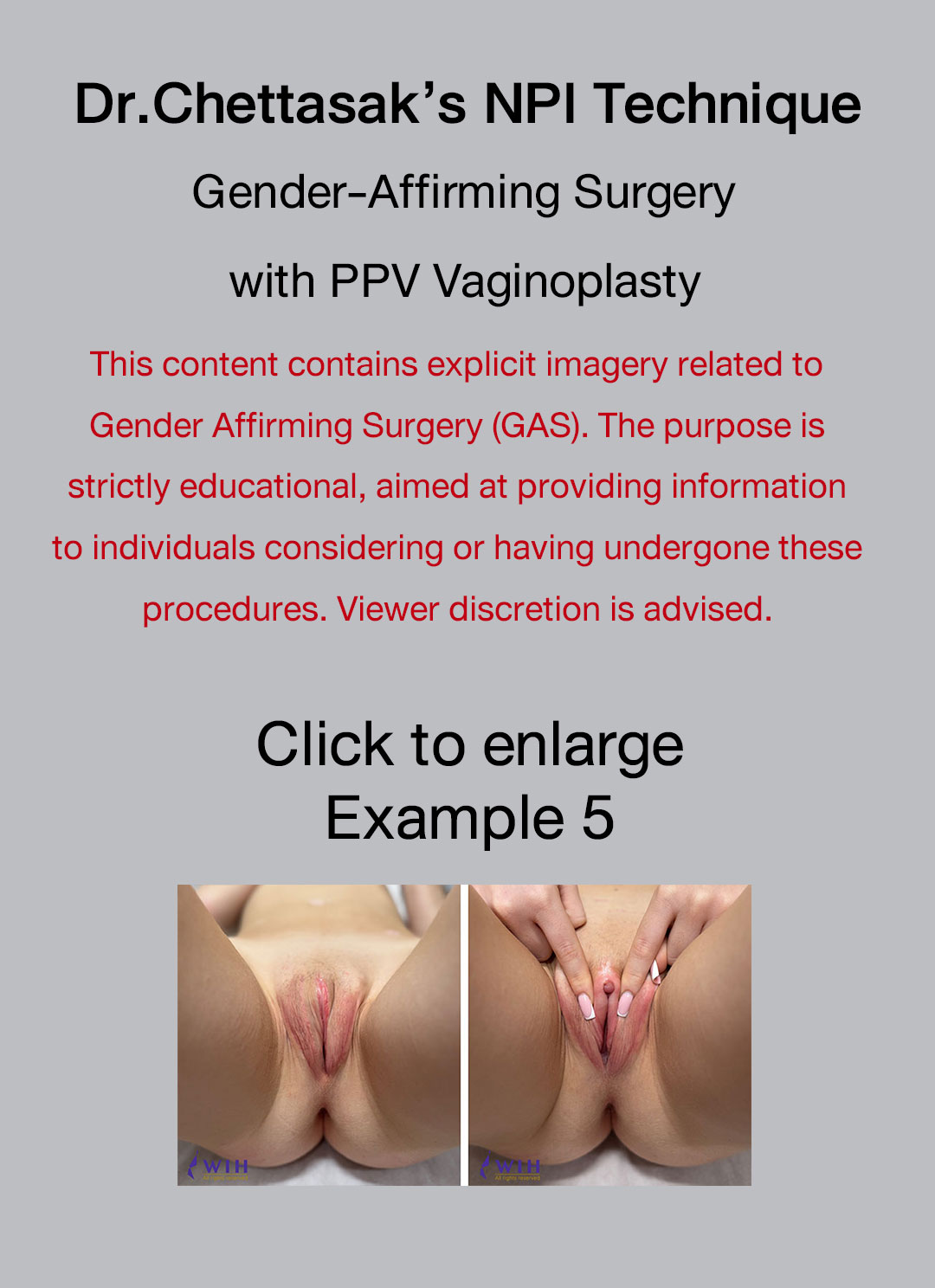
Surgical Procedure: Dr. Chettasak’s NPI Technique with Peritoneal Vaginoplasty
Dr. Chettasak Tulayaphanich performs this advanced procedure combining his signature NPI (Non-Penile Inversion) technique with Peritoneal Vaginoplasty to provide optimal aesthetic, sensory, and functional outcomes at WIH International Hospital.
Surgical Step: Dr. Chettasak’s NPI technique for external genitalia appearance
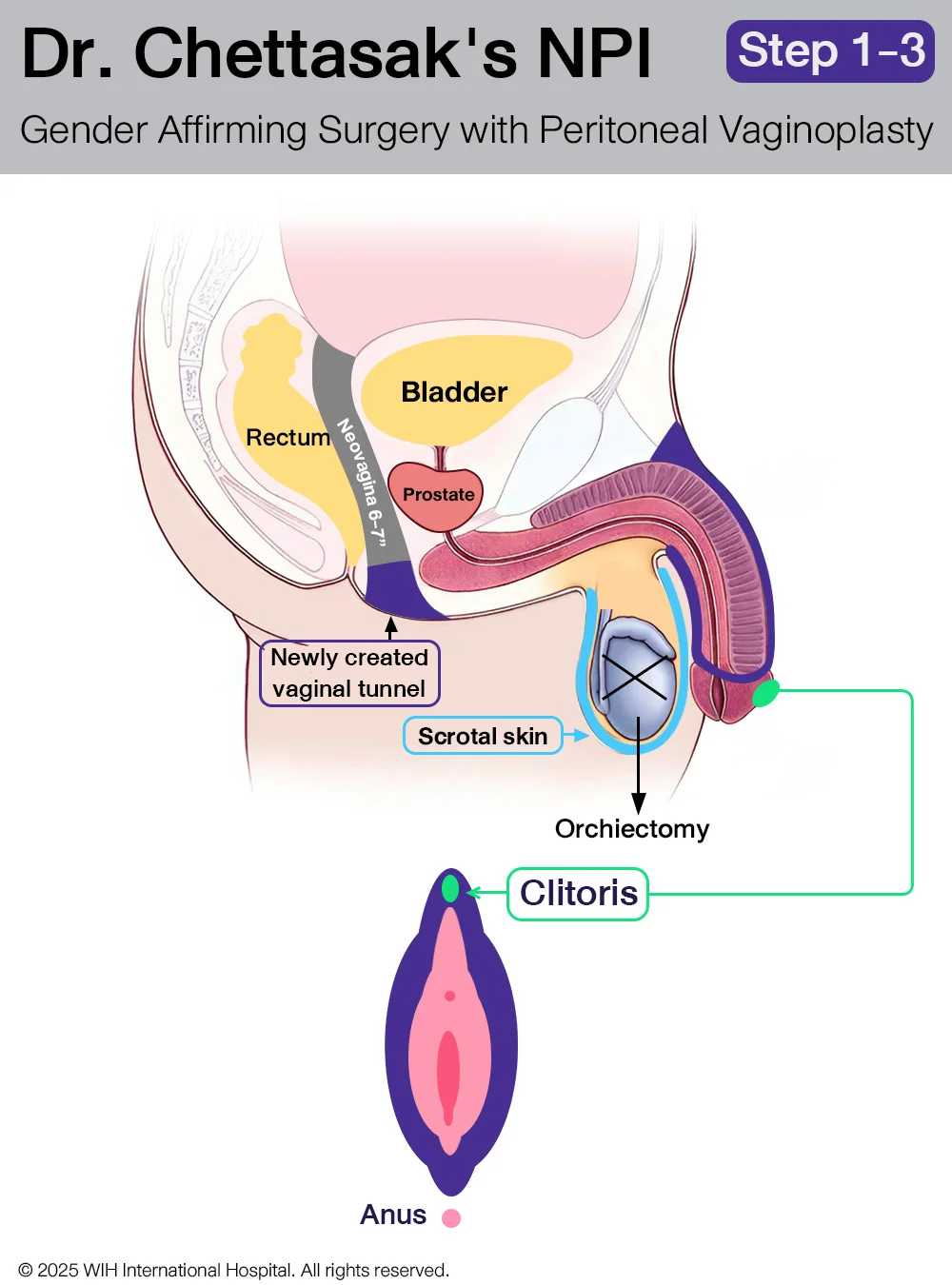
Step 1: Designing the Vaginal Opening and Creating the Tunnel
Dr. Chettasak begins by designing the vaginal opening, with careful incorporation of the perineal skin to form the floor of the new vaginal entrance. This approach enhances the natural appearance and structure of the vaginal introitus.
Next, a tunnel is meticulously created to follow the anatomical pathway of a natal female. This tunnel runs just beneath the urethra and behind the bladder, extending toward the posterior pelvic cavity, where it will later be connected to the abdominal cavity. This prepared space will receive the sigmoid colon segment during the next surgical phase.
Step 2: Bilateral Orchidectomies
Both testicles are surgically removed in a procedure known as bilateral orchidectomy. During this step, the entire spermatic cord is also carefully excised, with the cut made as close as possible to the external ring of the inguinal canal. This technique helps create a smoother contour in the groin area and reduces the risk of palpable remnants.
Importantly, the scrotal skin is preserved in optimal condition, as it will be used in the later stages to construct the outer labia (labia majora), ensuring a natural and feminine aesthetic outcome.
Step 3 : Clitoris and Clitoral Hood Reconstruction
The clitoris is reconstructed from the dorsal part of the glans penis, using a precise dissection technique to maintain maximum sensory function. Dr. Chettasak meticulously preserves the clitoral neurovascular pedicle, ensuring the branches of the pudendal nerve remain intact to support long-term erogenous sensation.
To provide an aesthetically natural appearance, the clitoral hood is created using a portion of the prepuce skin, mimicking the protective fold of tissue found in natal female anatomy. This step not only enhances the appearance but also helps reduce direct friction on the clitoris, contributing to postoperative comfort and sexual function.
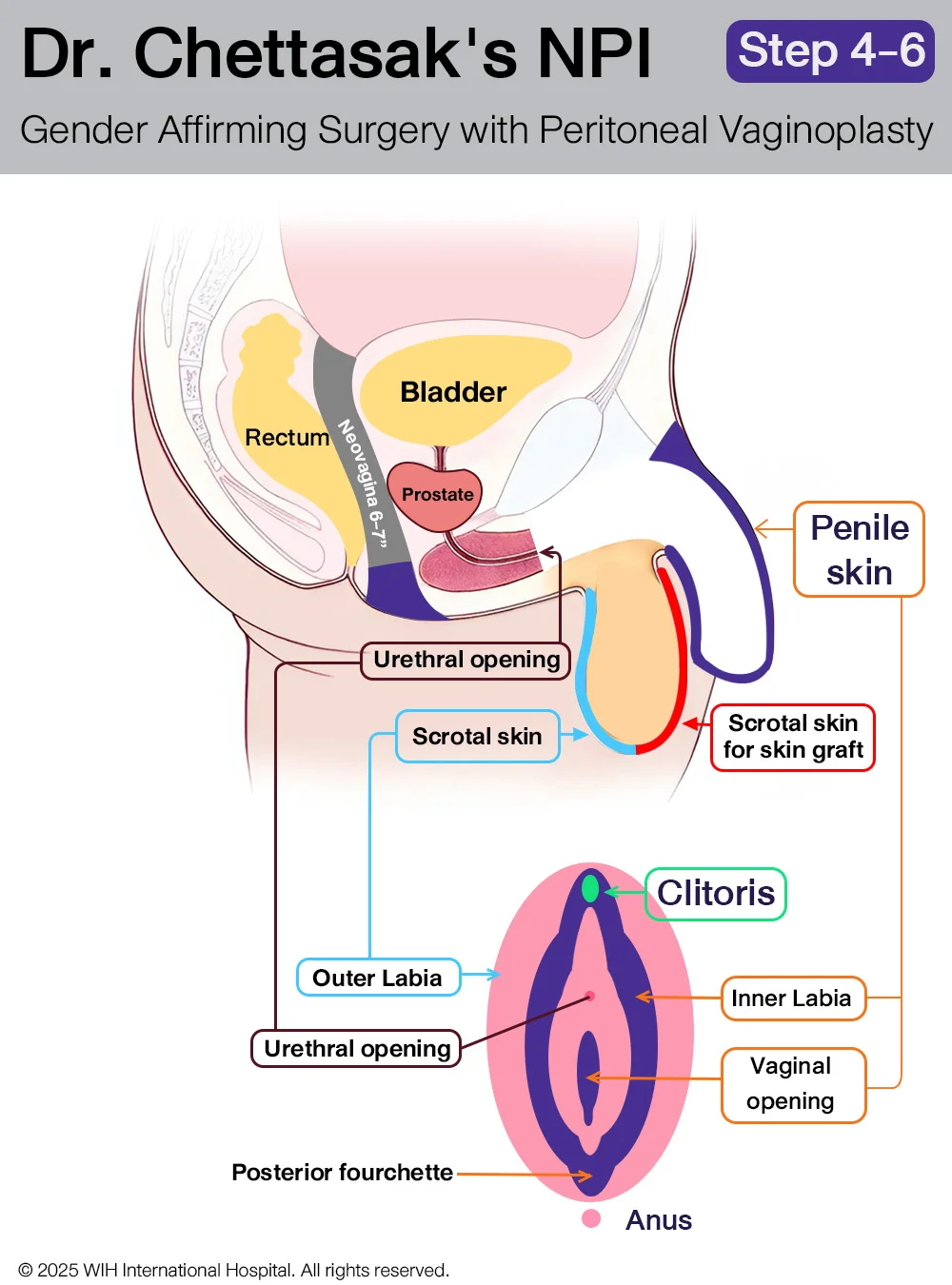
Step 4: Penectomy and Urethral Reconstruction with Penile Skin Preservation
The penis is removed through a careful penectomy, during which the entire corpus spongiosum—the spongy tissue surrounding the urethra—is also completely excised to prevent residual erectile tissue and improve surgical precision.
At the same time, the urethra is shortened and repositioned to align with typical female anatomy. A new urethral opening is reconstructed just above the introitus (vaginal entrance) to mimic the natural female location.
Throughout this step, Dr. Chettasak Tulayaphanich ensures that the penile and prepuce skin are preserved in optimal condition. These tissues will be used in the following step to create the inner labia and a natural-looking vaginal opening as part of Dr. Chettasak’s signature NPI technique.
Step 5: Inner Labia, Vaginal Opening, and Posterior Fourchette Reconstruction
Using the preserved penile and prepuce skin, Dr. Chettasak Tulayaphanich carefully reconstructs the inner labia and sculpts a natural-looking vaginal opening with a delicate V-contour. This approach ensures a feminine and realistic appearance.
A key part of this step is the precise creation of the posterior fourchette—the natural joining point at the lower end of the vaginal opening—using the inner folds of preserved skin. This detail enhances both the aesthetic and anatomical authenticity of the vagina.
This reconstruction method is the signature feature of Dr. Chettasak’s Non-Penile Inversion (NPI) technique, which is globally recognized for delivering superior cosmetic and sensory outcomes in gender-affirming surgery.
Step 6: Outer Labia Reconstruction
The outer labia are reconstructed using the preserved scrotal skin, completing the external genital reconstruction phase.
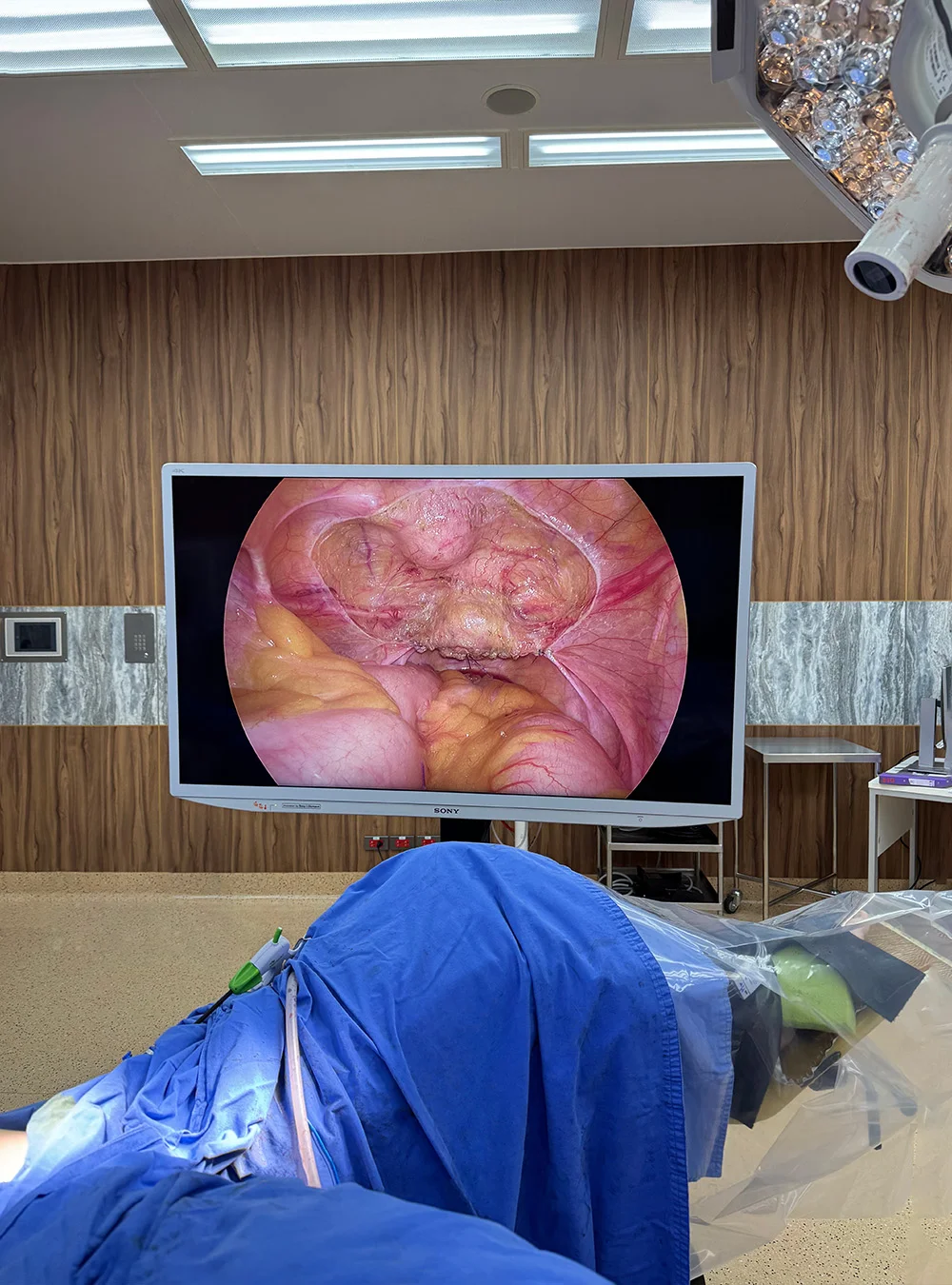
Surgical Step: Peritoneal Flap Harvest and Hybrid Neovaginal Reconstruction in PPV Vaginoplasty
In Dr. Chettasak’s hybrid technique of Peritoneal Pull-through Vaginoplasty (PPV), the neovaginal canal is constructed using a distal skin graft and a proximal peritoneal flap, which are seamlessly joined to create a single continuous neovaginal lining.
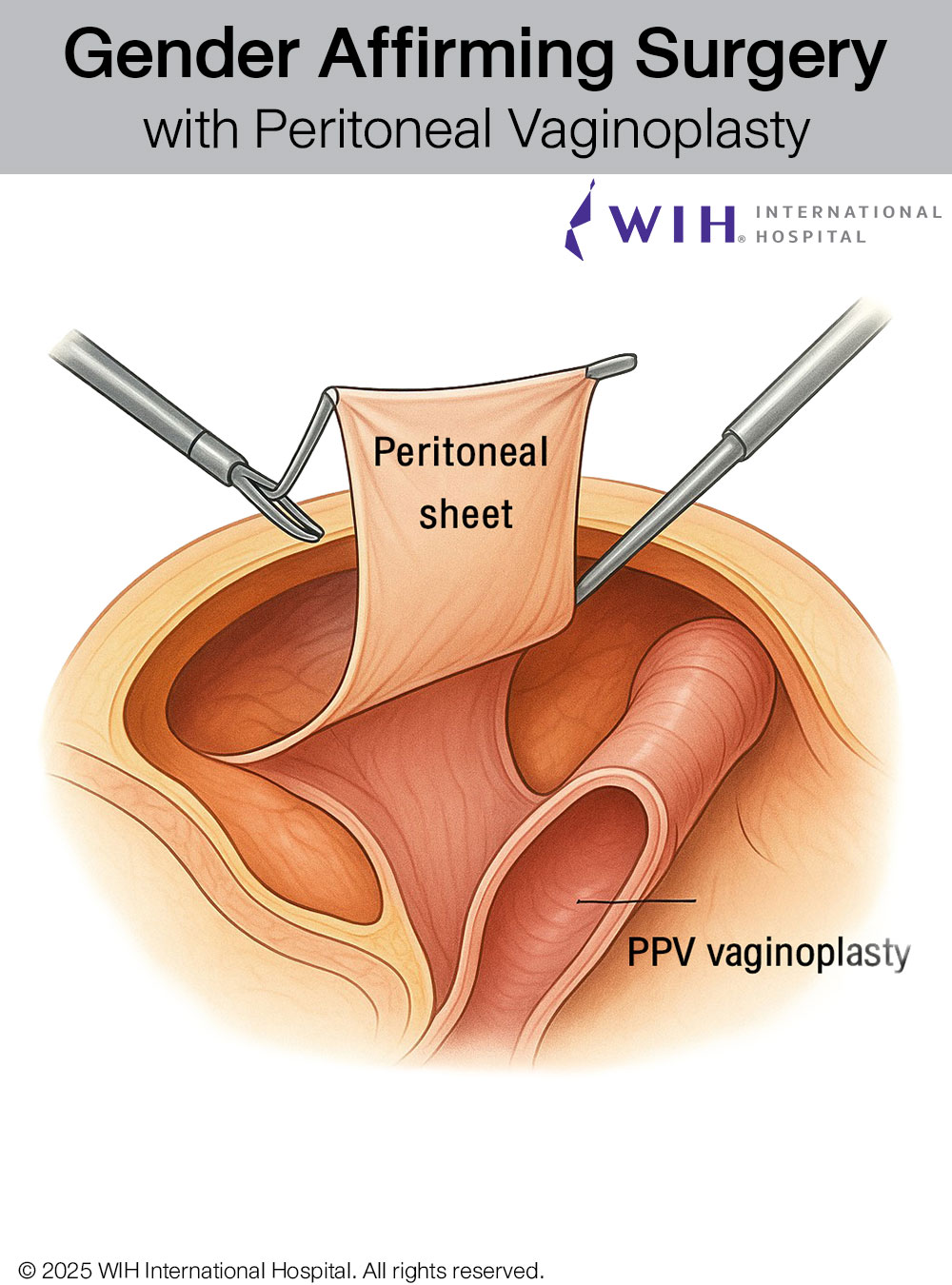
The procedure begins with laparoscopic access through three small (1 cm) incisions: one at the umbilicus and two in the lower abdominal quadrants. The abdominal cavity is insufflated with CO₂ to create a safe and spacious working field. The anterior peritoneum overlying the lower abdominal wall and bladder dome is carefully inspected and selected for flap harvest due to its elasticity and vascular reliability.
A rectangular peritoneal flap is designed individually for each patient, with the size carefully calculated to obtain the maximum usable area while preserving tissue perfusion. Dissection is performed using sharp technique and bipolar cautery, taking care to preserve subperitoneal vessels and avoid injury to the bladder and inferior epigastric vessels.
Once harvested, the peritoneal flap is folded into a pouch and delivered into a neovaginal tunnel created from the perineum. The distal portion of the canal is lined with skin graft, while the proximal canal is lined with the peritoneal pouch. The two components are joined internally with absorbable barbed sutures (e.g., V-Loc™) to ensure a smooth, continuous channel. The proximal flap is also anchored to pelvic tissues to prevent migration or retraction.

Step 1: Patient Preparation and Positioning
- Patient placed in lithotomy position
- Administration of general anesthesia
- Sterile preparation of surgical field

Step 2: Creation of Vaginal Canal Space
- Dissection between rectum and urethra/bladder
- Careful separation to create adequate space for neovagina

Step 3: Peritoneal Harvesting
- Laparoscopic access to abdominal cavity
- Identification and mobilization of peritoneal flap
- Careful preservation of blood supply to peritoneal tissue
Step 4: Peritoneal Pull-Through
- Transfer of peritoneal flap to vaginal canal space
- Suturing of peritoneal tissue to create vaginal lining
- Formation of vaginal apex/cuff
This hybrid approach offers:
- A soft, moist neovaginal lining with peritoneal tissue
- Durable distal coverage using skin graft
- Minimally invasive harvest through only three 1 cm incisions
- Aesthetic and functional outcomes with individualized flap design
Expert Care at WIH Hospital
At WIH Hospital, Dr. Chettasak and our multidisciplinary surgical team offer advanced laparoscopic-assisted PPV with a focus on safety, aesthetics, and function. Each procedure is customized based on the patient’s anatomy, goals, and tissue availability to ensure optimal long-term outcomes.
Following surgery, patients are required to continue with daily vaginal dilation by the WIH Hospital Vaginal Dilation Schedule Protocol. Strict adherence to this schedule is essential for maintaining neovaginal depth, preventing tissue contraction, and ensuring the long-term success of the surgery.
→ To learn more or consult about your surgical options, visit the
Gender-Affirming Surgery Center or contact our patient care team.
Book Your Transformation Today – Consult with Our Specialists


Other Interesting Articles
Optional Vaginal Dilation Program: 50+50+50 = 150 Minutes a Day
Three sessions of 50 minutes (morning, afternoon/early evening, before bed) suits patients who are home
17
Jul
Jul
4 Things You Should Avoid After Shoulder Narrowing Surgery
What Is Shoulder Narrowing Surgery and Why Is It Becoming Popular? a procedure designed to
05
May
May

Transition and Real-Life Experience
Transition refers to the steps an individual takes to live in a gender role that
22
Oct
Oct

Historical Castration vs. Modern Orchidectomy
Learn how modern, WPATH-approved orchidectomy by Dr. Chettasak differs from the painful
17
Sep
Sep

Pulmonary Embolism (PE)
Learn about pulmonary embolism (PE), causes, symptoms, diagnosis, and treatment. WIH Hospital provides expert
26
Aug
Aug

Ontario OHIP Coverage for Vaginoplasty and Revision Surgery
Discover OHIP funding for gender-affirming surgeries in Ontario. Learn about eligibility, application steps
23
Aug
Aug

Pixie Ear (elf ear surgery)
Correcting pixie ear at WIH Hospital with expert surgeons. Learn causes, treatments, and surgical repair
23
Aug
Aug

A Step-by-Step Breast Massage Guide
As you move into the recovery phase, one of the most crucial steps for achieving
19
Aug
Aug